Lauren MacGuidwin
Product designer
Connecting patients to primary care
Overview
I led vision, design, research, and testing for Solv’s first primary care product, including patient-facing provider detail pages, electronic health record (EHR) integration, ratings / reviews, and paperwork. It led to $500,000+ in revenue and 9,500+ appointment bookings across 200+ providers.
Team
I worked closely with a product manager, engineering manager, and a small team of engineers over the course of one year.
Challenge
Solv was an urgent care marketplace in which patients could browse clinics and book visits, while providers and operators could boost patient volume and experience. Leadership wanted to break into the larger primary care market to increase revenue and build the vision of a universal healthcare marketplace.
Research
I conducted interviews with primary care practices and patients. Practices wanted a full but efficient appointment schedule, relying heavily on their electronic health record (EHR) for scheduling and managing patient information. Patients wanted a provider who is in-network, competent, caring, and convenient, relying heavily on word-of-mouth and reviews to find high-quality providers.
Product vision
I led a cross-functional workshop, organized common themes, and presented our new product vision to build alignment and excitement across the team.

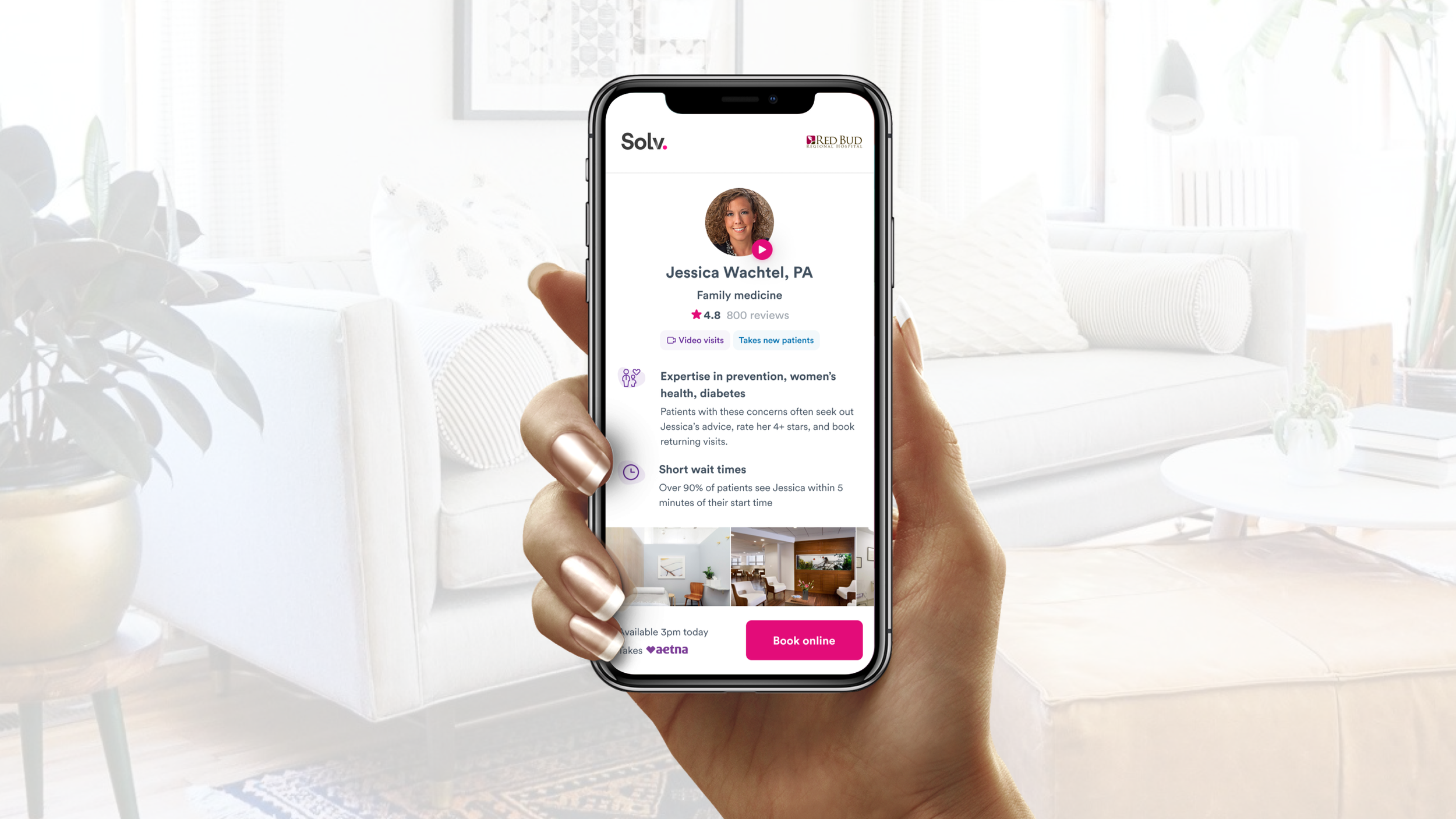
Appointment schedules and surfacing time slots
Patients valued seeing bookable time slots, but primary care schedules were much more complex than urgent care, often accommodating multiple providers with different schedules, locations, visit types, and paperwork requirements.
Since appointment availability could differ based on the patient and visit type, I explored whether to show a pre-screener to reveal the correct time slots or surface time slots by setting smart, but editable, defaults.
A) Pre-screening questions before showing time slots
B) Surface time slots with smart defaults
After gathering feedback from product reviews, user testing, and our client partner, we chose direction B since we could reasonably assume most people would be new patients seeking a new patient visit.
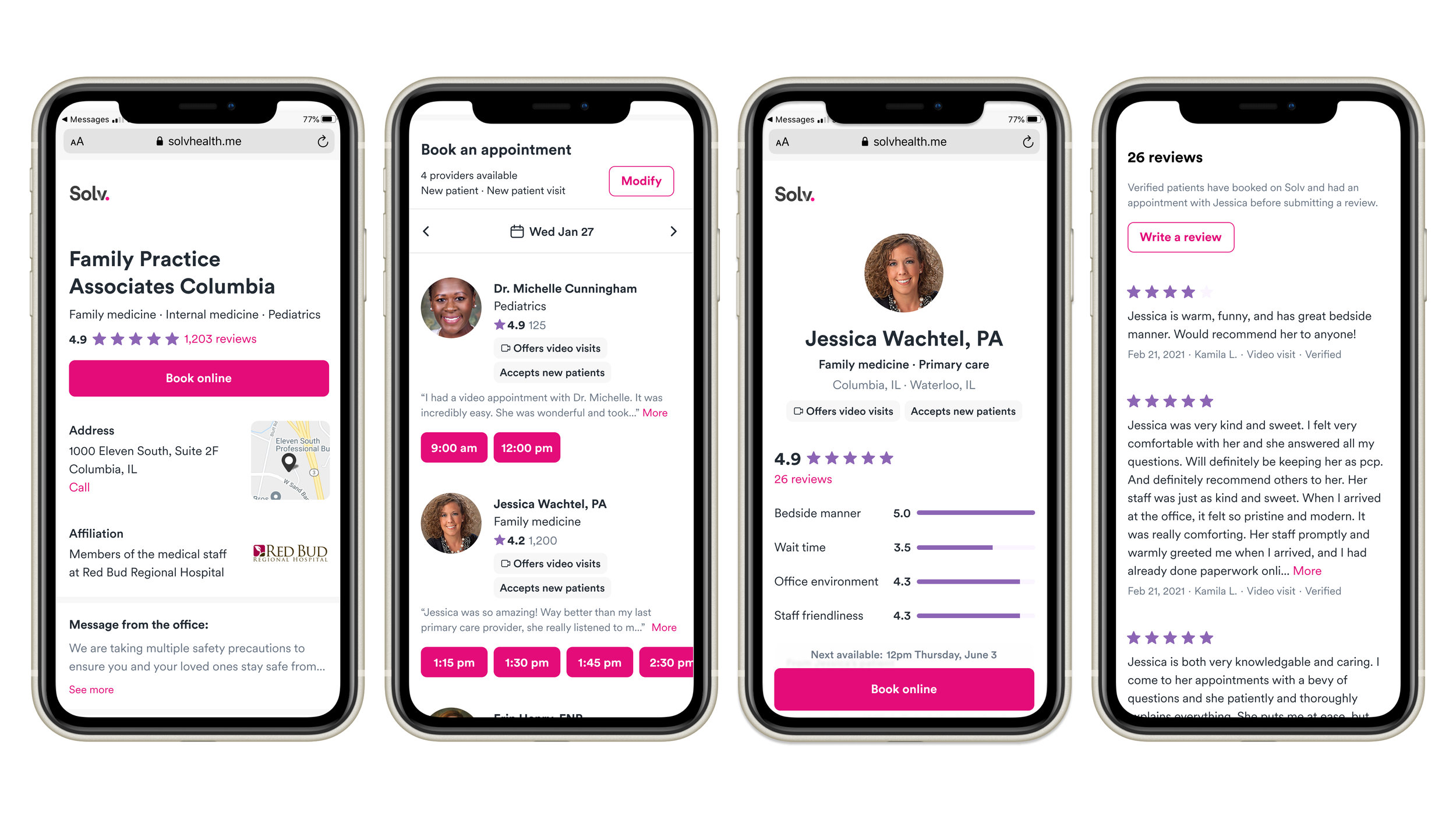
Attracting new patients with ratings & reviews
Our initial launch received positive feedback from our partner and prospects, but we needed to increase traffic through SEO improvements and reviews. I audited existing online review content, tested ratings categories, and refined with user testing feedback.
User testing respondents found the ratings and reviews sections easy to use and valuable for deciding on a provider. After testing, I made adjustments to the wait time UI (wasn’t prominent enough), and removed the filter and sort tooling (wasn’t in scope for engineering timelines).
Enhancing paperwork for primary care needs
Sales feedback revealed our paperwork product, which had been adapted from urgent care flows, wasn’t comprehensive enough for primary care needs. I worked with product, sales, and our chief medical officer to create a more robust set of paperwork questions. Since intake would be much longer, I tested whether asking one question per page could improve users’ sense of progress and chance of completion.
“All of these things are really important for a physician for someone who’s treating me medically. They’d need to know these things. For me personally, I don’t have problems providing that information.”
Respondents found this framework clear and intuitive, and furthermore, believed its comprehensiveness was a benefit, not a burden, to their healthcare experience.
Leveling up the org
Along the way, I implemented a new design system, a design documentation library, a research and testing guide, and an onboarding guide to improve the speed, quality, and impact of the tech org.
An end-to-end walkthrough of provider pages, booking, and paperwork.
Outcome
The product received $500,000+ in annual recurring revenue, 9,500+ appointment bookings for 200+ providers, and positive qualitative feedback from partners. Our primary care paperwork completion rates were more than double that of urgent care, even though the length was much longer.
“Lauren is a thoughtful and collaborative design partner who not only consistently delivers high-quality work, but also inspires those around her to do better.”